首页 > 医疗资讯/ 正文
[摘要]背景与目的:准确定位肺结节是胸腔镜手术成功的关键。本研究旨在探讨胸腔镜下外科手术治疗位于叶间胸膜下近肺门特殊位置肺结节的策略并评估其可行性、安全性及临床价值。方法:本研究收集2023年5月—2024年11月在聊城市肿瘤防治院行肺结节外科手术的患者,对于不符合纳入标准的患者予以排除。本研究获聊城市肿瘤防治院伦理委员会批准(伦理编号:EC-20240112-1020)且获得患者知情同意。本研究是前瞻性单臂研究,对纳入的患者采取CT引导下经叶间胸膜穿刺定位肺结节的非常规穿刺定位方式,进而对其行楔形切除术,评价术前CT引导下定位术的成功率及并发症发生率,分析围手术期并发症,验证此类手术方式的可行性。结果:本研究共纳入28例符合入组标准的患者。男性5例,女性23例,年龄38~69岁,平均(56.0±8.5)岁。对28例患者合计28个结节行胸腔镜楔形切除术,术前CT引导下定位全部成功(100.0%),无需要紧急处理的并发症。胸腔镜手术平均时间为(15.6±4.0) min;术中出血(20.9±14.3)mL,术后引流(214.3±62.2) mL,漏气0例,中转开胸手术0例;住院平均时间为(5.4±0.9)d。肺结节术后病理学检查结果为良性的患者有3例,其中肺组织纤维化2例,非典型腺瘤样增生1例;恶性有25例,其中原位腺癌5例,微浸润性腺癌16例,浸润性腺癌4例。结论:通过CT引导下经过叶间胸膜定位肺结节并行胸腔镜楔形切除,既可保证手术切除的准确性,最大可能地切除肿瘤,同时又避免了肺段或者肺叶切除造成正常肺组织损失,安全快捷,对于此类特殊位置肺结节的手术治疗具有重要的指导意义。
[关键词] 肺结节;楔形切除术;CT引导;过叶间裂定位
[Abstract] Background and purpose: Accurately locating pulmonary nodules is the key to the success of thoracoscopic surgery. This study aimed to investigate the strategy and evaluate the feasibility, safety, and clinical value of thoracoscopic surgical treatment for pulmonary nodules located beneath the interlobar pleura and close to the pulmonary hilum. Methods: The patients who underwent pulmonary nodule surgery at Liaocheng Tumor Hospital from May 2023 to November 2024 were enrolled, and the patients who did not meet the inclusion criteria were excluded. This study was approved by the Ethics Committee of Liaocheng Tumor Hospital (EC-20240112-1020) and informed consent was obtained from the patients. The research was designed as a prospective single-arm study. The patients were treated with wedge rep, which was performed following CT-guided localization, where the location needle was inserted through the interlobar pleura. The feasibility of the procedure was evaluated by analyzing the success rate of preoperative localization and perioperative complications. Results: A total of 28 patients who met the inclusion criteria were included in this study. There were 5 male and 23 female patients with an average age of (56.0±8.5) years (range 38-69 years). In all, 28 patients with 28 nodules underwent thoracoscopic wedge rep, and the preoperative CT-guided localization was successfully performed in all patients, without urgent complications. The mean operation time of thoracoscopic surgery was (15.6±4.0) min, intraoperative bleeding was (20.9±14.3) mL, and postoperative drainage was (214.3±62.2) mL. No cases of postoperative air leaks or conversion to thoracotomy were observed. The average length of hospital stay was (5.4±0.9) days. The postoperative histological diagnosis revealed 3 benign lesions (pulmonary fibrosis in 2 cases, atypical adenomatous hyperplasia in 1 case) and 25 malignant lesions (adenocarcinoma in situ in 5 cases, minimally invasive adenocarcinoma in 16 cases, and invasive adenocarcinoma in 4 cases). Conclusion: Thoracoscopic wedge rep following CT-guided nodule localization through the interlobar pleura is a feasible approach for nodules located beneath the interlobar pleura and close to the pulmonary hilum. The method ensures precise tumor localization, adequate margin, and minimal loss of normal lung tissue, with a low incidence of postoperative complication, which has important guiding significance for the surgical treatment of pulmonary nodules in such special locations.
[Keywords] Pulmonary nodules; Thoracoscopic wedge rep; CT guidance; Located through the interlobar pleura
随着多层螺旋CT的广泛应用,肺结节检出率逐年升高,部分肺结节经术后病理学检查证实为早期肺癌。电视辅助胸腔镜手术(video-assisted thoracic surgery,VATS)具有操作时间短、创伤小、患者术后恢复快等优点,已成为治疗肺结节的重要手段。准确定位肺结节是胸腔镜手术成功的关键,术前在CT引导下对肺结节进行准确定位,可以明确肺结节位置及其与周围组织的关系,从而在手术中更精确地切除病灶,减少手术创伤,提高手术的安全性和成功率。部分肺结节位于叶间胸膜下且距肺门较近,常规定位方式难度大,外科需进行肺段乃至肺叶切除才能完全切除病灶,切除的肺组织多,创伤较大,并发症多,患者术后恢复慢。针对这种特殊位置的肺结节,本前瞻性单臂研究在CT引导下经过叶间胸膜定位并对患者行胸腔镜楔形切除术,进而评估此治疗策略的可行性、安全性及临床价值。
1 资料和方法
1.1 一般资料
本研究收集2023年5月—2024年11月在聊城市肿瘤防治院行肺结节外科手术的患者。本研究患者的纳入标准为:① 术前行薄层CT扫描发现肺结节位于肺门附近且位于叶间胸膜下;② 患者可接受手术治疗;③ 术前行CT引导下过叶间裂肺结节定位。排除标准:① 肺结节位置不符合上述标准;② 有手术禁忌证者;③ 术前未行肺结节定位。本研究为前瞻性单臂研究,经聊城市肿瘤防治院伦理委员会批准(伦理编号:EC-20240112-1020)。所有患者均已在聊城市肿瘤防治院获得知情同意。
1.2 仪器与方法
使用东软医疗系统股份有限公司生产的128层螺旋CT,120 KV,270 mA,螺距0.9,转速0.6秒/圈,FOV 30~35 cm,矩阵512×512,肺算法重建,重建层厚/层间距1 mm。穿刺针采用一次性使用肺结节定位穿刺针[MFA-1-10,镁格生物科技(江苏)有限公司]。根据术前CT图像所示结节位置选择合适的患者体位(仰卧、俯卧或侧卧),在无痛清醒静脉麻醉下(咪达唑仑2 mg静脉推注,纳布啡4 mg静脉推注)行CT引导下穿刺定位。根据结节位置,选择穿过叶间裂作为穿刺路径(图1A),确定皮肤进针点。消毒铺无菌洞巾后,在皮肤进针点以2%利多卡因行局部浸润麻醉。经过分步穿刺及多次CT扫描验证,定位针达结节外侧,释放定位针,拔出推送装置,固定定位线,CT扫描验证定位针置于肺结节旁(图1B),测量定位针与结节的距离(L)并观察有无并发症及是否需要处理。按术前设计方案于全身麻醉下行VATS楔形切除术或剥除术。
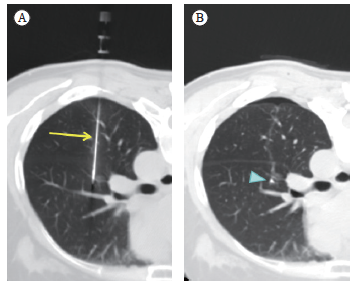
图1 CT引导下过叶间裂定位肺结节
Fig. 1 CT guided localization of pulmonary nodules through the interlobar pleura
A: Localization of nodules in the posterior segment of the upper lobe through oblique pleural in the posterior segment of the lower lobe (yellow arrow for puncture guidance needle); B: A few pneumothorax and needle bleeding occurred after positioning surgery (the blue triangle refered to the positioning needle).
2 结 果
2.1 患者资料
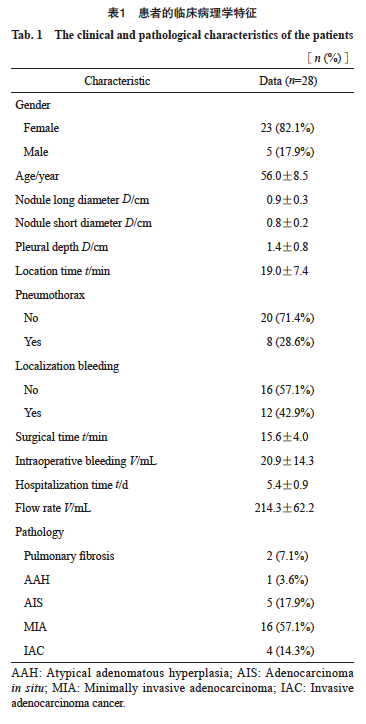
共有159例患者纳入了初步研究。其中,120例患者肺结节不位于肺门附近的叶间胸膜下。在剩余的39例患者中,有5例患者有手术禁忌证、 6例患者术前未行CT引导下过叶间裂肺结节定位方案而被排除在外,最终28例患者纳入本研究,纳入和排除标准流程图见图2。本研究共纳入了28例患者进行研究,其中男性5例,女性23例,年龄38~69岁,平均(56.0±8.5)岁。患者的基本特征见表1。
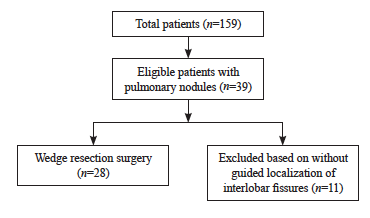
图2 患者纳入和排除流程图
Fig. 2 Patient s’ inclusion and exclusion flowchart
2.2 定位及手术治疗结果
定位及手术切除范围示意图见图3。手术操作:于腋前线至腋中线6或7肋间做一长约4 cm切口作为观察孔及操作孔,置入切口保护套,使用超声刀打开叶间裂,定位线从一叶肺组织穿出,经叶间裂穿入另一叶肺组织(图4A),以定位线穿入点为标记向内侧延伸测量距离(L)精确确定结节位置。超声刀充分游离近端气管、血管及定位针附近肺组织(图4B),楔形切除或剥除包括结节及定位针在内的肺组织(图4C),标本送术中快速冰冻切片病理学检查(图4D、E)。
手术共切除28枚肺结节,结节长径0.5~ 1.7 cm,平均(0.9±0.3)cm;病灶均位于肺门附近、叶间胸膜下,距离胸膜0.5~3.5 cm,平均(1.4±0.8)cm。28个结节均成功行CT引导下经叶间裂定位,定位成功率为100.0%(28/28),定位时间8~36 min,平均(19.0±7.4)min。在穿刺过程中,12例(12/28,42.9%)穿刺针道附近轻微渗血,8例(8/28,28.6%)出现轻度气胸,出气量均<5%;同时发生气胸和渗血者3例(3/28,10.7%),均未予特殊处理。
28例患者均在定位后接受肺结节胸腔镜楔形切除术,术中均按定位针指示成功地找到并切除病灶。胸腔镜进入胸腔后均清晰可见位于胸膜腔的定位线,28枚结节的定位线均穿过叶间裂位于肺内。胸腔镜楔形切除单个结节耗时8~25 min,平均(15.6±4.0)min,术中出血(20.9± 14.3)mL,术后引流(214.3±62.2)mL,漏气0例,中转开胸手术0例,平均住院时间为(5.4±0.9)d。术中均送快速病理学检查,病理学检查结果现实良性3例(3/28,10.7%),包括肺组织纤维化2例(2/28,7.1%),非典型腺瘤样增生(atypical adenomatous hyperplasia,AAH)1例(1/28,3.6%)。恶性共25例(25/28,89.3%),包括原位腺癌(adenocarcinoma in situ,AIS)5例(5/28,17.9%),微浸润性腺癌(minimally invasive adenocarcinoma,MIA)16例(16/28,57.1%),浸润性腺癌(invasive adenocarcinoma cancer,IAC)4例(4/28,14.3%)。患者的临床病理学特征见表1。
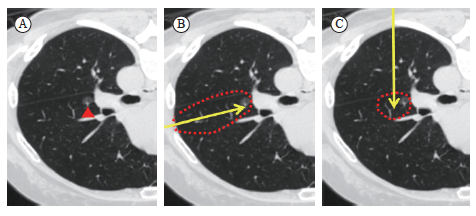
图3 定位及手术切除范围示意图
Fig. 3 Schematic diagram of positioning and surgical rep range
A: Surgical rep of subpleural ground glass nodule (red triangle) in the upper lobe of the left lung; B: Schematic diagram of needle insertion around small nodules through lateral chest wall puncture (yellow arrow represents the puncture needle path,the red dashed line represents the surgical rep range); C: Schematic diagram of needle insertion through the dorsal segment of the lower lobe to reach the outer side of the small nodule (yellow arrow represents the puncture needle path, the red dashed line represents the surgical rep range).
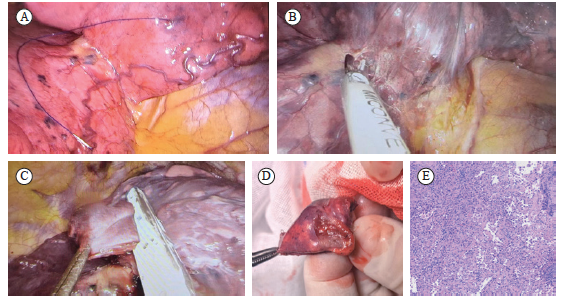
图4 根据定位针指引楔形切除肺结节
Fig. 4 Wedge rep of pulmonary nodules guided by positioning needle
A: The positioning line passes through one lung tissue, and the positioning needle is located beneath the pleura of the other lung tissue; B: Ultrasound knife free proximal trachea, blood vessels, and lung tissue near the positioning needle; C: Wedge rep of lung tissue including nodules and positioning needles; D: Lung tissue specimen; E: Pathological image (MIA).
3 讨 论
肺癌是死亡率最高的恶性肿瘤[1]。随着低剂量胸部CT筛查的广泛应用,越来越多的以磨玻璃(ground-glass opacity,GGO)为主要表现的肺癌被及时检出[2],其中绝大多数是肺腺癌,根据2019年国际肺癌研究协会(International Association for the Study of Lung Cancer,IASLC)、美国胸科学会(American Thoracic Society,ATS)及欧洲呼吸学会(European Respiratory Society,ERS)国际多学科肺腺癌新分类标准所提出的肺腺癌病理学分类标准[3],肺腺癌可分为原位腺癌、微浸润性腺癌及浸润性腺癌3种。早期肺癌的传统手术方式是肺叶切除联合纵隔淋巴结清扫术,由于GGO型肺腺癌惰性生长特性及患者良好的长期生存情况,传统根治性肺叶切除联合系统性纵隔淋巴结清扫术已经不再适用于部分早期肺腺癌患者[4]。肺癌手术的原则是最大限度地切除病变组织以及最大限度地保留正常肺组织。有学者指出肺癌微创3.0的概念[5],即以器官微创为核心,整合切口微创和系统微创,最终实现使患者生存期更长、生活质量更高的目标,为减少早期肺癌患者手术创伤提供了新方向。对于Ⅰ期周围型肺腺癌患者,对原位腺癌/微浸润性腺癌的患者仅行亚肺叶切除,不清扫纵隔淋巴结,其5年无复发生存率(recurrence-free survival,RFS)达100%[6-7]。日本临床肿瘤学组织(Japan Clinical Oncology Group,JCOG)0804研究[8]指出,薄层CT最大肿瘤直径≤2 cm并且实性/肿瘤比率(consolidation tumor ratio,CTR)≤0.25的GGO病灶行亚肺叶切除术患者的5年RFS达99.7%,也同样证实了上述结论。而CALGB140503临床研究[9]则探究了亚肺叶切除与肺叶切除对治疗周围型ⅠA期非小细胞肺癌的效果,结果表明,亚肺叶切除术的术后生存不劣于肺叶切除术,且能为患者保留更好的肺功能,因此,足够切缘的亚肺叶切除术应该是GGO占优势的周围型肺肿瘤≤2.0 cm者首选的手术方式。亚肺叶切除包括楔形切除和肺段切除,在两者均可的情况下,如果肿瘤位置允许,楔形切除是首选的手术方式[5]。对于接受楔形切除即可达到治愈结果的肺癌患者人群,进行肺段切除术可能属于“过度治疗”的范畴,无端地增加了患者的治疗创伤[10]。肺楔形切除术因其手术时间较短且能够保留更多的正常肺组织而越来越受到重视。
浸润前肺腺癌(包括原位腺癌和微浸润性腺癌)往往表现为亚实性小结节,与周围肺组织难以区分,术中无法利用胸腔镜器械触摸到结节, CT引导下肺结节定位可协助手术准确定位,提高手术精准度,帮助判断足够切缘,尽可能保留更多健康肺组织,缩短手术时间[6]。位于叶间胸膜下且近肺门的结节,常规穿刺路径穿刺针只经过单叶肺组织将定位针置于结节附近。如按此种定位方式,手术须进行肺段切除甚至肺叶切除,会切除过多的正常肺组织,创伤较大,肺功能损失较多,造成过度治疗[11]。如果采取过叶间裂穿刺进针,穿刺针将经过两个肺叶到达结节附近,虽然进针路径较长,但外科可进行楔形切除,能保留更多的正常肺组织。此种定位方式穿刺路径长,且穿过三层胸膜,出血及气胸的发生率增加,尤其是当穿刺针经过叶间裂胸膜时,一旦发生气胸造成肺组织萎陷,将给精确定位造成困难[12]。所以在设计穿刺路径时,既要选择最短路径,又要注意避开大血管,同时穿刺针过胸膜时进针要迅速,避免在胸膜上停留,可以减少并发症的出现。本研究28例患者28个结节均成功行CT引导下经叶间裂定位,部分患者出现轻微气胸及针道渗血,均未出现大出血及严重气胸,定位成功率为100%。28例结节均行楔形切除,其中3例良性,21例为浸润前肺腺癌。浸润前肺腺癌患者无论接受何种手术切除方式,其10年的RFS均可达100%[13-15]。4例术中快速冰冻病理学检查诊断为微浸润性腺癌,但术后石蜡包埋组织切片病理学检查结果为浸润性腺癌,因其最大径小于2 cm,且CTR≤0.25,接受楔形切除术后的5年RFS仍达100%[16],所以楔形切除术可满足临床要求。采用楔形切除术作为治疗手段,相较于传统的肺段切除术或肺叶切除术,能够最大程度地保留肺功能,减少手术对患者生活质量的影响,显示出其先进性。这种手术方式在保留患者肺功能的同时,也为治疗早期肺癌提供了新的思路。
但本研究也存在局限性:① 本研究只收集28例患者,样本数量少,结果可能存在偏倚,还需进一步收集病例进行研究;② 随访时间短,没有5年总生存及5年RFS等长期随访数据,还需进一步追踪随访,这些都是后期仍需进一步探究和解决的问题。
综上所述,对位于叶间胸膜下且近肺门的特殊位置肺结节,可以采取经过叶间裂胸膜定位的非常规穿刺定位方式,对其行楔形切除术。这种外科治疗策略既可以保证手术切除肿瘤的准确性及完整性,也可以最大限度地减少正常肺组织的损失,避免过度治疗,且术后并发症发生率更低,住院时间更短,能更好地保留患者的肺功能,真正实现患者长期高质量生存的目标。
并列第一作者:
吴雯丽,副主任医师, CT室副主任;宋庆平,副主任医师,胸外科主任。
通信作者:
姜峰,副主任医师,胸外科副主任;
作者贡献声明:
吴雯丽:撰写文章;宋庆平:修改文章;耿东晓:收集数据;赵燕风:分析整理数据;陈海泉:设计研究方案,论文指导;于秋凤:文献查阅和整理;姜峰:研究选题,论文审核。
[参考文献]
[1] SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249.
[2] VLAHOS I, STEFANIDIS K, SHEARD S, et al. Lung cancer screening: nodule identification and characterization[J]. Transl Lung Cancer Res, 2018, 7(3): 288-303.
[3] TRAVIS W D, BRAMBILLA E, NOGUCHI M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society: International multidisciplinary classification of lung adenocarcinoma: executive summary[J]. Proc Am Thorac Soc, 2011, 8(5): 381-385.
[4] 邓朝强, 张 宁, 傅方求, 等. 肺癌微创3.0的再认识和实践[J]. 临床外科杂志, 2022, 30(8): 701-704.
DENG C Q, ZHANG N, FU F Q, et al. Re-understanding and practice of minimally invasive 3.0 for lung cancer[J]. J Clin Surg, 2022, 30(8): 701-704.
[5] CHENG X H, ONAITIS M W, et al. Minimally invasive thoracic surgery 3.0: lessons learned from the history of lung cancer surgery[J]. Ann Surg, 2018, 267(1): 37-38.
[6] YE T, WU H X, WANG S P, et al. Radiologic identification of pathologic tumor invasion in patients with lung adenocarcinoma[J]. JAMA Netw Open, 2023, 6(10): e2337889.
[7] 李 宁, 吴 鹏, 申郁冰, 等. 2020-2030年中国4种主要癌症相关死亡率的预测[J]. 癌症, 2022, 41(1): 8-17.
LI N, WU P, SHEN Y B, et al. Prediction of four major cancerrelated mortality rates in China from 2020 to 2030[J]. Chin J Cancer, 2022, 41(1): 8-17.
[8] SUZUKI K, WATANABE S I, WAKABAYASHI M, et al. A single-arm study of sublobar rep for ground-glass opacity dominant peripheral lung cancer[J]. J Thorac Cardiovasc Surg, 2022, 163(1): 289-301.e2.
[9] ALTORKI N, WANG X F, KOZONO D, et al. Lobar or sublobar rep for peripheral stage ⅠA non-small cell lung cancer[J]. N Engl J Med, 2023, 388(6): 489-498.
[10] 钱 斌, 陈海泉. 2023年度肺癌外科治疗领域重要进展[J]. 中国癌症杂志, 2024, 34(4): 335-339.
QIAN B, CHEN H Q. Important progress in surgical treatment of lung cancer in 2023[J]. Chin Oncol, 2024, 34(4): 335-339.
[11] 吴雯丽, 赵燕风, 唐 威, 等. 气胸风险预测模型在CT引导下肺穿刺活检术中的验证研究[J]. 医学影像学杂志, 2022, 32(10): 1693-1697.
WU W L, ZHAO Y F, TANG W, et al. Validation study of pneumothorax risk prediction model in computed tomography guided percutaneous core needle biopsy of the lung[J]. J Med Imag, 2022, 32(10): 1693-1697.
[12] 傅方求, 张 扬, 陈海泉. 如何认识和理解肺腺癌外科治愈窗口期[J]. 中国胸心血管外科临床杂志, 2023, 30(12): 1674-1677.
FU F Q, ZHANG Y, CHEN H Q. The surgical curative time window for lung adenocarcinoma: a comprehensive understanding[J]. Chin J Clin Thorac Cardiovasc Surg, 2023, 30(12): 1674-1677.
[13] LI D, DENG C Q, WANG S P, et al. Ten-year follow-up results of pure ground-glass opacity-featured lung adenocarcinomas after surgery[J]. Ann Thorac Surg, 2023, 116(2): 230-237.
[14] LI D, DENG C Q, WANG S P, et al. Ten-year follow-up of lung cancer patients with resected adenocarcinoma in situ or minimally invasive adenocarcinoma: wedge rep is curative[J]. J Thorac Cardiovasc Surg, 2022, 164(6): 1614-1622.e1.
[15] YOTSUKURA M, ASAMURA H, MOTOI N, et al. Long-term prognosis of patients with resected adenocarcinoma in situ and minimally invasive adenocarcinoma of the lung[J]. J Thorac Oncol, 2021, 16(8): 1312-1320.
[16] ZHANG Y, DENG C Q, FU F Q, et al. Excellent prognosis of patients with invasive lung adenocarcinomas during surgery misdiagnosed as atypical adenomatous hyperplasia, adenocarcinoma in situ, or minimally invasive adenocarcinoma by frozen p[J]. Chest, 2021, 159(3): 1265-1272.
- 搜索
-
- 1000℃Nutrients:真实世界数据,纤维肌痛患者的饮食与运动自适应规律
- 1000℃D-二聚体升高诊治与管理专家共识(2026)
- 1000℃专家论坛|文良志:门静脉血栓的诊断和治疗
- 1000℃首例儿童NF2驱动型胸膜间皮瘤,多方法学检测锁定NF2双等位基因失活和14/22号染色体缺失,提示与成人胸膜间皮瘤不同
- 1000℃打破误区:干扰素追求CHB功能性治愈,HBsAg为何“不降反增”?
- 1000℃迷惑性极强的肝内病灶!影像表现疑点重重,最终病理竟查出两种不同肝脏恶性肿瘤
- 1000℃指南共识|原发性肝癌分子靶向药物相关蛋白尿中西医结合诊疗专家共识
- 1000℃Diabetologia:意大利北部社区 1~100 岁人群胰岛自身抗体与乳糜泻 TGA-IgA 的年龄分布及检测方法学验证
- 精J Child Psychol Psychiatry:12种罕见神经发育障碍儿童沟通能力谱系
- 精研究发现:爱吃辣的人,心血管病和癌症死亡风险都会显著降低
- 精Nursing in Critical Care:别再指责护士了!ICU 里被遗漏的护理,根源在系统而非个人
- 精Acta Obstet Gynecol Scand:罕见病女性的妊娠并发症与母婴结局,一项单中心434种罕见病的回顾性队列研究
- 精【爱儿小醉】儿科患者术前对流层臭氧暴露与围手术期呼吸系统不良事件之间的关系:一项单中心回顾性队列研究
- 精eBioMedicine:牙龈下微生物组与脑健康存在连续关联梯度,牙周炎或成认知衰退可干预靶点
- 精军事医学研究院《自然·通讯》:自适应IrPtCu纳米酶水凝胶实现耐药菌感染伤口序贯治疗
- 精能够逆转萎缩性胃炎的两个中成药,该怎么选择?
- 荐同时性多发性原发性肺癌,左右病灶分别为EGFR和ALK阳性,考虑淋巴结肿大仅局限左肺门及血浆EGFR阳性,采用奥希替尼联合化疗
- 荐40岁女性同时罹患卵巢支持细胞-间质细胞瘤和透明细胞乳头状肾肿瘤,WES等基因检测竟为阴性
- 荐椎管内麻醉使用止血药突发气道痉挛的抢救流程解析
- 荐女子肝区无任何不适,影像提示复杂囊性病变,层层鉴别后锁定罕见胆管源性囊性肿瘤
- 荐“绘”真报告 | 病理考虑为中枢神经细胞瘤,检出脑室外神经细胞瘤的特征性变异FGFR1-TACC1融合,辅助鉴别诊断
- 荐8岁女童出现男性化症状,竟是形似「性索-间质肿瘤」的卵巢「无性细胞瘤」所致,少见KRAS/CDK4共扩增或与侵袭性有关
- 荐17例病例分析揭示常见于中年人的色素性室管膜瘤临床特征与预后,分子检测可助力临床精准诊疗
- 荐Lancet Oncol:结直肠癌腹膜转移,围手术期化疗并非必选项
- 标签列表
-
- 星座 (702)
- 孩子 (526)
- 恋爱 (505)
- 婴儿车 (390)
- 宝宝 (328)
- 狮子座 (313)
- 金牛座 (313)
- 摩羯座 (302)
- 白羊座 (301)
- 天蝎座 (294)
- 巨蟹座 (289)
- 双子座 (289)
- 处女座 (285)
- 天秤座 (276)
- 双鱼座 (268)
- 婴儿 (265)
- 水瓶座 (260)
- 射手座 (239)
- 不完美妈妈 (173)
- 跳槽那些事儿 (168)
- baby (140)
- 女婴 (132)
- 生肖 (129)
- 女儿 (129)
- 民警 (127)
- 狮子 (105)
- NBA (101)
- 家长 (97)
- 怀孕 (95)
- 儿童 (93)
- 交警 (89)
- 孕妇 (77)
- 儿子 (75)
- Angelababy (74)
- 父母 (74)
- 幼儿园 (73)
- 医院 (69)
- 童车 (66)
- 女子 (60)
- 郑州 (58)